1. What is the most likely diagnosis? A. Osteosarcoma B. Paget’s disease C. Fibrous dysplasia D. Calvarial metastases E. Subgaleal hematoma Show correct answer
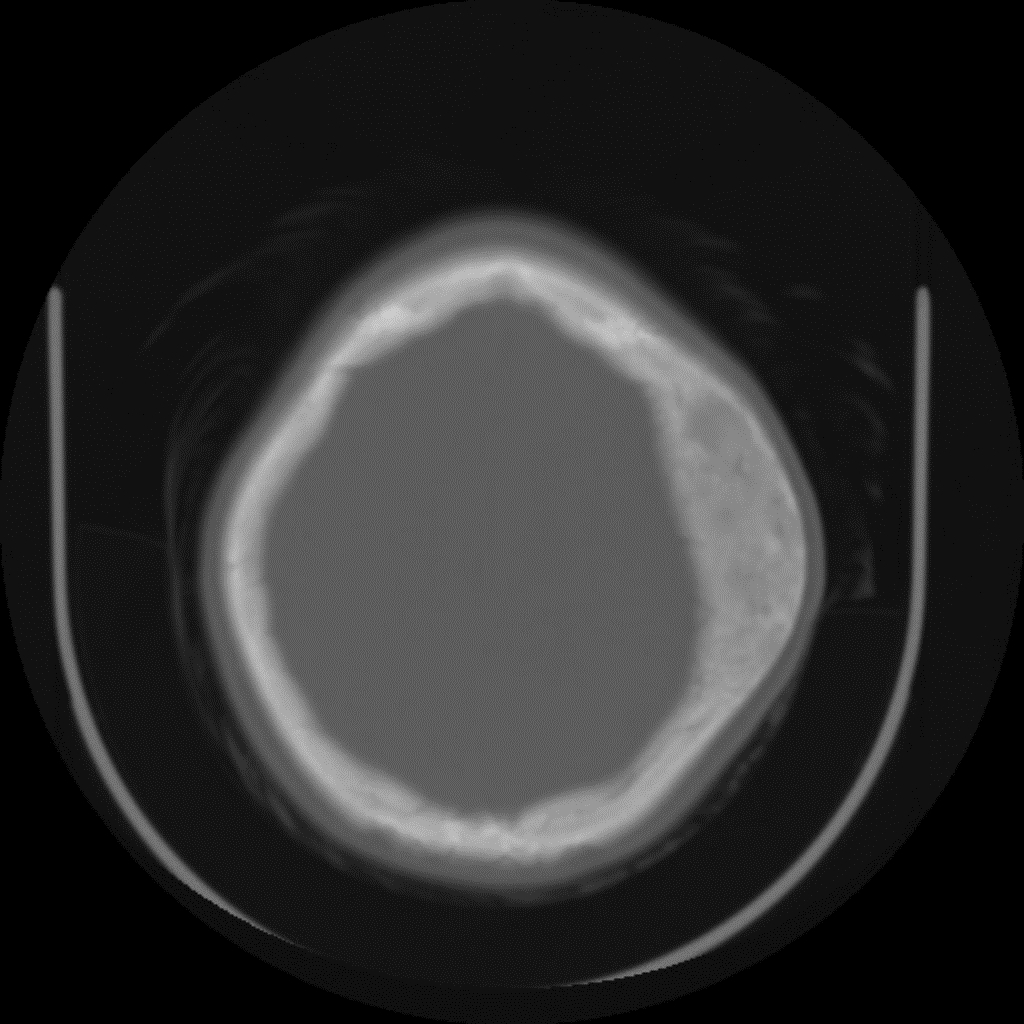
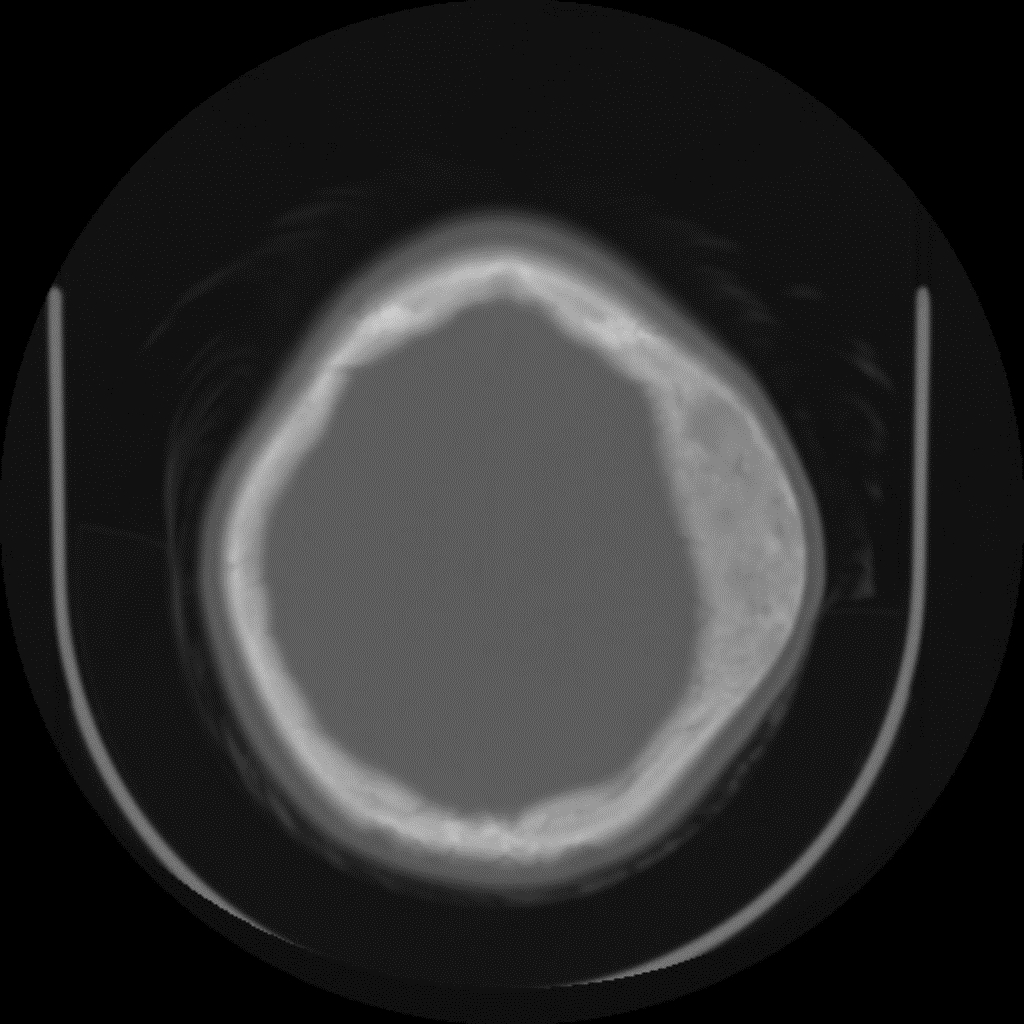
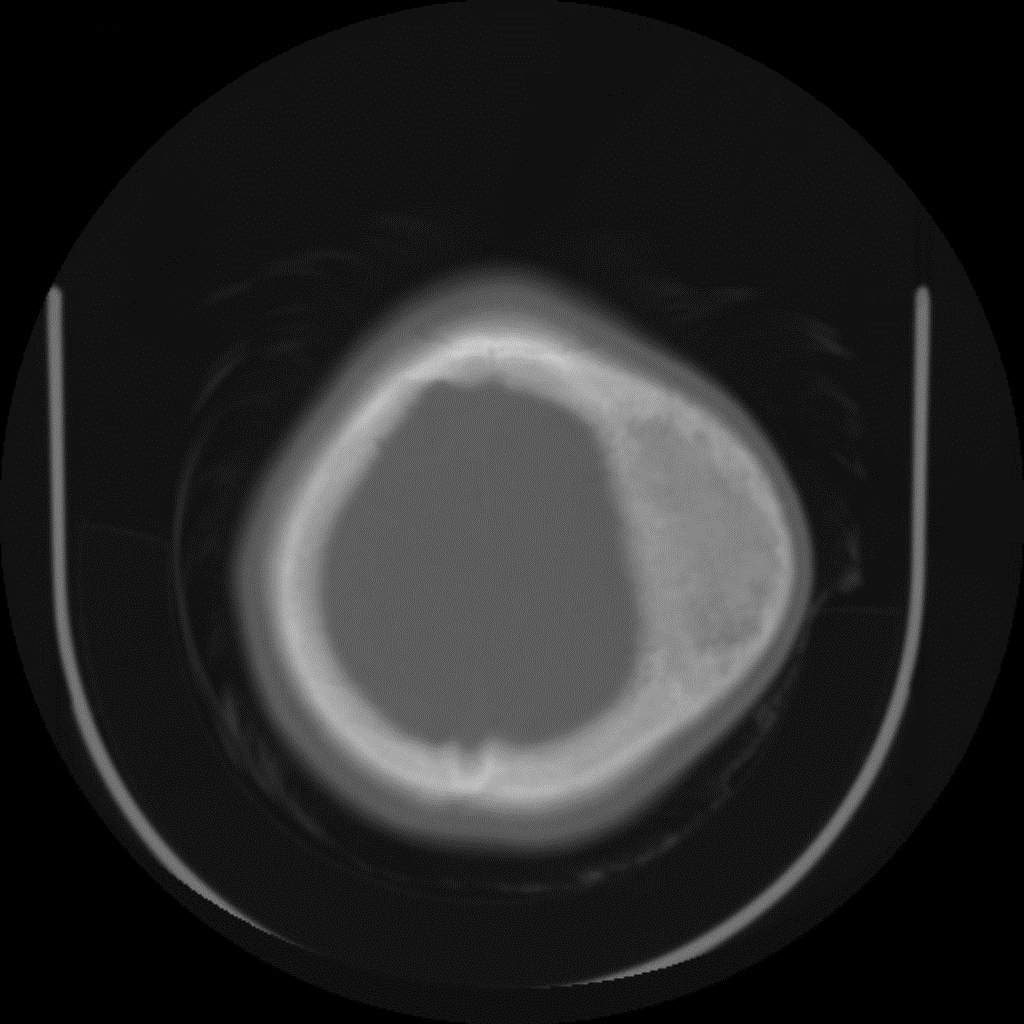
A. Incorrect. The lesions as shown in figure 1-6 shows benign features (well defined margins, no periosteal reaction, no cortical destruction)
B. Incorrect. Paget’s disease is found in adults, not children.
C. Correct. The expansile lesion shown in figure 1-6 demonstrates ground glass appearance which is a characteristic of fibrous dysplasia.
D. Incorrect
E. Incorrect
Next Question »
2. In relation to facial involvement of fibrous dysplasia, which statement is false? A. The mandible is more common involved than the maxilla. B. Involvement of facial bones is more commonly found in the polyostotic form than in the monoostotic form. C. Cranial nerve palsy is one of the manifestations of fibrous dysplasia. D. Mucoceles have been reported related to fibrous dysplasia in facial bone. E. A transformation to osteosarcoma, fibrosarcoma or chondrosarcoma is rare. Show correct answer
A. incorrect answer. The maxilla is more commonly involved than the mandible in fibrous dysplasia.
B. correct answer. Fibrous dysplasia, an idiopathic benign fibro-osseous disorder, may be monostotic, polyostotic, or part of McCune-Albrigth syndrome (polyostotic fibrous dysplasia, café-au-lait-pigmentation, and sexual precocity in a female). Involvement of the facial bones and skull is more common in the polyostotic form.
C. incorrect answer. An expansion of the bone may narrow the spinal canal or neural foramina of the skull base. This may compress or entrap cranial nerves and result in cranial nerve palsy.
D. incorrect answer. Osteo-meatal obstruction by expansion of the bone may lead to a mucocele.
E. incorrect answer. There is a 0.5-1% incidence of malignant transformations, predominately osteosarcoma, fibrosarcoma and chondrosarcoma. The malignant tansformation is more often seen in the polyostotic form than in the monostotic form. Increasing pain, an enlarging soft tissue mass or a previously mineralized lesion that becomes lytic should raise suspicious for malignant transformation.
« Previous QuestionNext Question »
3. In relation to fibrous dysplasia, which statement is false? A. On T1WI, the signal intensity of fibrous dysplasia is similar to that of the skeletal muscle. B. On T2WI, the signal intensity of fibrous dysplasia is variable, hyper- or hypointense. C. Fluid-fluid levels have been described in fibrous dysplasia. D. Soft tissue extension is common in fibrous dysplasia. E. Peripheral enhancement may be seen after gadolinium administration. Show correct answer
A. True.
B. True. Although the signal of pure fibrous tissue is hypointense on T2WI, that of fibrous dysplasia is variable.
C. True. A Fluid-fluid level has been described in fibrous dysplasias with cystic components.
D. False. Soft tissue extension of the lesion is unusual.
E. True. After gadolinium administration central, or less frequently, peripheral enhancement may occur.
« Previous Question
Show discussion
Discussion:
CT findings of fibrous dysplasia involving craniofacial bones include areas of homogeneously increased density with bone thickening that give a relatively radiopaque appearance (some references called this the ‘compact form’). These lesions are found most frequently at the base of the skull and involve the sphenoid body, the orbital roof and the lesser wing of the sphenoid. The cranial vault frequently shows relatively radiolucent osteolytic lesions (some references call this the ‘lytic form’) and only 5% of cases show extensive involvement of the skull base.
The imaging findings of fibrous dysplasia have been well described by means of scintigraphy, radiography and CT. The MRI features of fibrous dysplasia show low signal intensity on T1-weighted images, while the signal intensity on T2-weighted images varies from high to intermediate or low signal. This variation may reflect the overall cellularity, collagen content, extent of the bone trabeculae and cyst formation. Jee et al described MR findings in fibrous dysplasia of 38% hypointense lesions and 62% hyperintense lesions on T2 weighted images. Histopathologic examination of T2-hyperintense lesions revealed fewer bony trabeculae, less celluarity and fewer collagen fibers than the T2-hypointerse lesions. Metabolically more active lesions also demonstrate prolonged T2 relaxation times, similar to that seen in other actively growing tissues.
References:
1. Robson CD, Kim FM, Barnes PD. Head and neck. In: Kirks DR, Griscom NT. Practical pediatric imaging: diagnostic radiology of infants and children. Philadelphia: Lippincott-Raven Publisher, 1998:225.
2. Dahnert W. Bone and soft tissue disorders. In: Dahnert W. Radiology review manual. Philadelphia: Lippincott Williams and Wilkins, 1996:63.
3. Fletcher BD. Benign and malignant bone tumors. In: Kuhn JP, Slovis TL, Haller JO. Caffey’s pediatric diagnostic imaging. Philadelphia: Mosby, 2003:2387
4. Swischuk LE. Head, brain and meninges. In: Swischuk LE, eds. Imaging of the newborn, infant and young child. Maryland: Willianms and Wilkins, 1997:1007.
5. Yuceer N, Kutluhan A, Bekerecioglu, Arslan H, Akman. Polyostotic fibrous dysplasia with craniofacial localization presenting with frontal lobe compression in a 14-year-old girl. Acta Neurochair 1999;141: 203-7.
6. Sirvanci M, Karaman K, Onat L, Duran C, Ulusoy, OL. Monostotic fibrous dysplasia of the clivus MRI and CT findings. Neuroradiology 2002; 44: 847-50.