Discussion:
Slipping of the upper femoral epiphysis is most often observed in children between 10 and 16 years of age and is more common in boys than girls. The average age of onset is about 2 years earlier in girls than in boys, coinciding with the earlier bone maturation of girls. In about one-fourth of the cases both hips are affected. The prognosis in patients with SCFE is related to both the promptness of diagnosis and the degree of slipping. If the displacement is treated early, when slipping is minimal or mild, the results are usually very good. Chronic SCFE of moderate degree, if pinned in situ, will usually result in a good functional hip, albeit with some limitation of mobility. Severe SCFE requires extensive surgical reconstruction, is more prone to complications, and has a poor prognosis regarding future function. Osteonecrosis is a serious complication of slipped epiphysis that usually results in considerable disability. Another frequent complication is chondrolysis, or cartilage necrosis (cell death). The development of osteoarthritis later in life can also be a complication of slipped epiphysis, and is directly related to the severity of the slip.
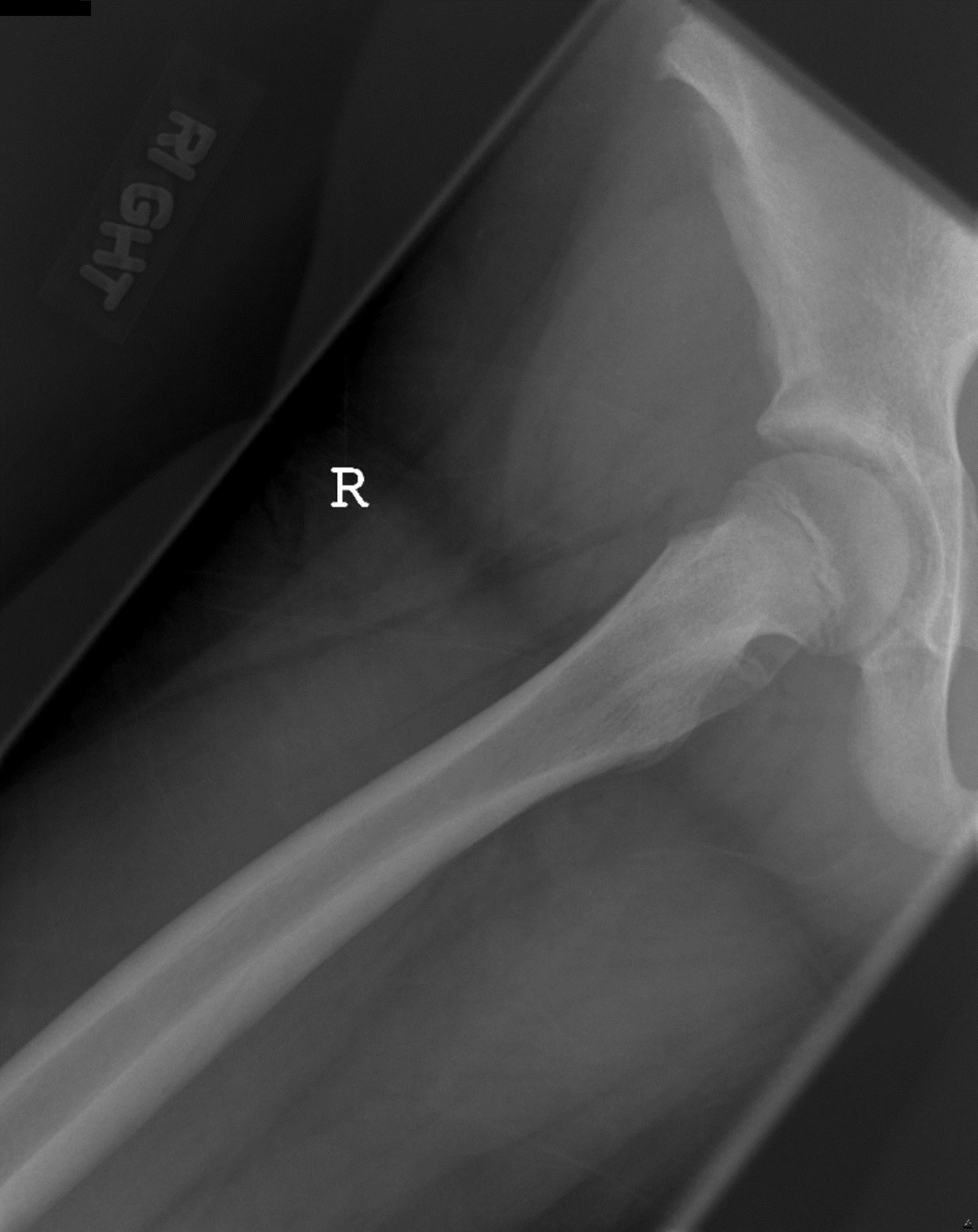
Sign of SCFE may be subtle on the frontal radiographs of the hips or pelvis. There is usually osteopenia of the femoral head and neck. The physis may be wide, and there is frequent blurring of its metaphyseal margin. A line drawn tangential to the lateral border of the femoral neck normally intersects with the epiphyseal ossification center, so that approximately one sixth of the diameter of the femoral head lies laterally to this line. In SCFE, the line along the femoral neck fails to intersect with the femoral epiphysis. There is frequently a displacement of the metaphysis from the acetabulum and a reduction in apparent epiphyseal height. Normally, on a true lateral or frog-lateral view, the anterior and posterior margins of the epiphysis and metaphysis match closely with a smooth junction. With SCFE, the lateral film shows a metaphyseal-epiphyseal discontinuity due to posterior displacement of the epiphysis.